- Trends
- Posts
- AI in Healthcare: How Providers are Using It
AI in Healthcare: How Providers are Using It
Some Non-Clinical Themes for AI Application in Healthcare
Paul Johnson
September 27, 2023
Generative AI became apparent to most of us in 2023. I remember first playing with new AI tools at about this time last year. I don’t think I slept well for a couple nights afterward — realizing how enormous its potential was.
While one specific application - ChatGPT - gets lots of the press right now, it is just one tiny part of the AI world. The concept of using large language models (LLMs) combined with a chat user interface are much larger than ChatGPT or its parent, OpenAI. For the sake of this writing, I call it all Generative AI – defined as the ability for AI to create new content based on inputs or the environment at that moment, and using natural language user interfaces, and learning from an LLM. In this way, generative AI is different than databases and tables, where the interface and output are both relatively pre-defined and static.
How Did We Get Here?
I’ve seen a few technological breakthroughs impact healthcare over my 27-year career. Some had staying power, some did not.
Early on, electronic health records created major change, but one could argue it was driven largely by regulation and has taken over 20 years to implement well.
Electronic remittance advices (e.g. 835s and 837s) changed a small portion of the healthcare world, but its benefits were really contained to those focusing on revenue cycle operations.
Blockchain was a buzzy topic for my clients back in 2019 and 2020, but the pandemic pretty much ended that shiny object syndrome.
Generative AI is the result of decades of development, which only recently became usable to the average person. Because it uses data that already exists – basically all the data we’ve ever created digitally – it is more of a new way of organizing and using information, and using it to create even new content. Generative AI feels different; It is being driven by the market and by users, and its applicability is obvious when you start to look under the hood.
Generative AI vs. Automation
The concept of automation or RPA is not new – in fact, I first started seeing inbound RPA-related requests from clients back in 2015. The ability to automate administrative processes, especially highly-repetitive one, is a material improvement for health systems. Nearly all have adopted some level of RPA deployment.
Where Generative AI takes it to a new level is in its ability to learn as the dataset grows, and our ability to interact with it using natural language.
Some of the use cases I provide below are rooted in “old-fashioned” (all of 8 years old!) automation, but are enhanced with today’s generative AI. It can be a blurry line between the two, but in most cases a classification is not needed. We can all just agree that the advancements lead to efficiency, and that is good.
Some AI Use Cases in Health Systems
How might Generative AI and LLMs impact healthcare? And when? There are a few things happening right now that may well impact the lives of a typical provider CEO, COO, CFO, or other executives, very quickly.
Since I am not a clinician, I won’t attempt to focus on clinical or therapeutic areas. Rather, here are a few of the performance improvement tasks I see GenAI having a near-term impact on.
Hiring and retention
Generative AI can have a direct impact on staff hiring and retention. Some of the early vendors are using AI to help healthcare systems identify top candidates from large candidate pools, using pattern-matching rather than static “check-box” criteria. This can be a more accurate way to winnow a pool of 300 candidates down to 10.
Training is an obvious area for AI, as you on-ramp employees. The idea of a “co-pilot” for every new app or tool that someone needs to learn will accelerate their learning curve. Unlike the old pop-ups or “search help” functions, chat-based AI can do it in a way that is highly-interactive and even predictive. For example, the system may know that you will likely have trouble with the next step, so it will jump in to guide you through it.
An intriguing use of AI right now, given the high demand for talent, is to identify staff who are at-risk of leaving your organization and improve retention. Some tools are being built to monitor patterns that suggest someone is about to quit. Perhaps they look at absentee rates, output, reporting relationships, time of year, and identify those who need a little extra boost.
Patient Throughput
To me, Scheduling is perhaps the most exciting and tangible near-term application of AI to our space. It starts with the ability to quickly match an inbound appointment request to the right provider, using all of a health system’s data and a chat-based conversation for what the patient needs. The AI can basically become a really smart patient router.
In the Peri-Op area, I’ve heard examples of developers working on the ability to be more predictive in scheduling. AI can look at historical patterns of OR scheduling, and know that Dr. Smith tends to not use her Friday block holds to the full extent, so those blocks should be offered to other surgeons a couple weeks out.
Still in the OR space, a good AI overlay on top of a scheduling and staffing systems can take the first pass at organizing the ORs for the next day…. schedules, staffing, supplies.
Finally, when looking at overall length-of-stay and discharge planning, Generative AI can compare your inhouse patients to all prior patients, and more specifically predict a patient’s discharge based on their condition and demographics. This could help eliminate the guessing game of which beds will open up each morning or afternoon. Based on a patient’s condition, diagnosis, demographic, and home situation, discharge planners can have a head start on getting each patient situated.
Early Adoption Areas: Documentation and Employee Services
Two areas where AI had been in the works for a while even prior to this year’s AI explosion, using natural language processing, are documentation and employee services.
Using voice-based AI to take the first pass at documentation can be a huge time-saver for physicians and APPs. This is a world apart from the old dictation, which still needed to be transcribed and documented. With AI-based documentation, the system not only synthesizes a note based on all of the information available in the system, but it also rounds-out any vague information or open questions based on comparing with other like, past patients.
Using chatbots in a real-time manner is also a feature for many employee service areas like HR or payroll. Because so many of the questions from employees are similar, I’ve had some clients suggest that a chatbot as the first line of response can reduce the number of questions requiring follow-up by 60% or more.
What About Startup Activity in This Space?
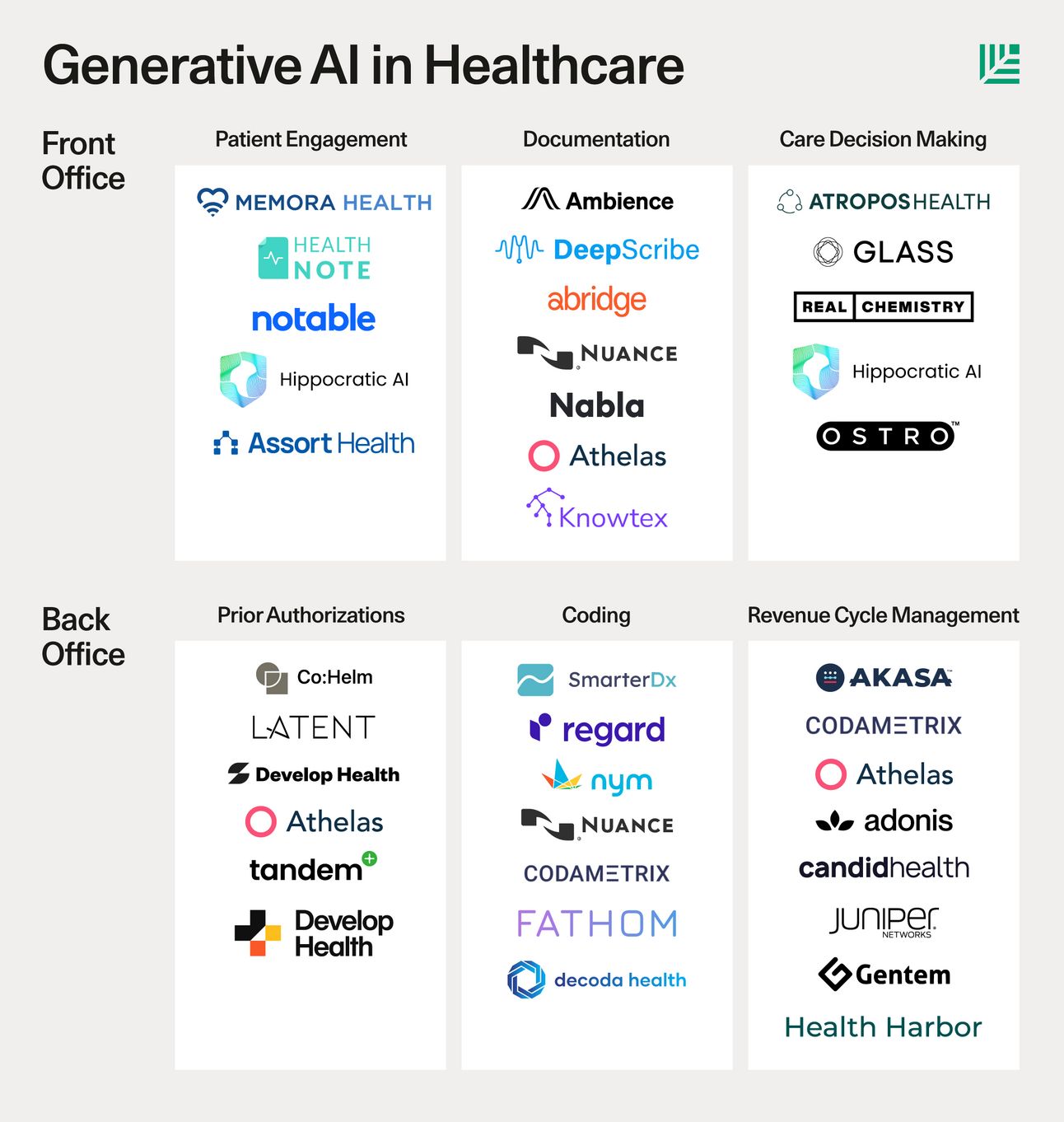
There is lots of startup activity emerging in the healthcare services AI space. I can’t endorse any of these companies, as I am not familiar with their execution, but it is good to see this type of innovative energy in the industry.
(Sequoia market map, late 2023)
So What are the Barriers to AI Adoption?
The promise of AI in our industry is so obvious, you might ask “What could possibly be a reason not to go all in?”
Governance is one potential barrier. Large organizations are rightfully worried about each department pursuing their own IA strategy, and ending up with a bunch of shadow systems overlapping like spaghetti. A new position I’ve started to hear about is a VP of AI who can provide central governance to the rollout. AI within an organization needs to be coherent, unified, leveraged, working toward organizational priorities.
Who owns the data? Because LLMs only get better with more data, they can be most powerful if you are combining the information of many organizations. However, given the level of privacy regulation in healthcare, along with the desire for a competitive advantage, data ownership within LLMs will be a point of focus in coming years.
Finally, Generative AI has been shown to have biases at first, as the data set often starts small and grows. If the AI is only “trained” on Medicare patients from the Midwest, for example, it may be blind to trends and patterns that exist in other patient demographics. The solution to AI bias is more data - and a larger LLM for it to learn from - but it takes a while to get there.
I can’t predict how this will all play out, but based on the early client work we are doing with AI, I am reminded of Bill Gates’ famous quote:
“We overestimate what will happen in 1 year, but underestimate what will happen in 10 years.